A new IBN is out. CFMO (Command Flight Medical Officer) support in reviewing Forms 6424 will be withdrawn in June with a deadline for new submissions at the end of April.
Seems that cadets who require a CFMO reviewed F6424 who do not already hold a one, or do not sort one before the deadline, will be unfit to fly until an alternative provision is made.
Impact on Cadet Flying and Gliding. Without medical assurance, those cadets declaring a medical condition on the AvMed 1, that requires F6424 action including CFMO review, will be considered as Unfit to Fly. RAFAC AvMed Form 1 will be amended to reflect the changes
So we’ll suddenly be in a situation where if you declare a medical problem, you just can’t fly. No opportunity to review, just a solid No.
I do wonder where this would sit us within the equality act. We can obviously ‘discriminate’ on medical grounds and tell cadets it’s not safe to fly. But the current system allows/shows that many of those who say yes can in fact fly. A blanket No without review arguably is quite discriminatory?
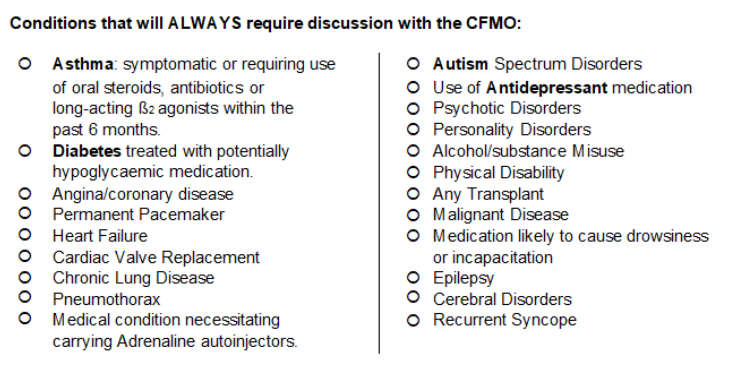
Not all F6424s necessarily require CFMO review, only those with conditions listed on the form as requiring review. But the list does contain some quite common conditions
Right, And that is a valid argument. Safety is a defence to discriminate, as it were.
But we currently have a system in place that works, so we have proven there are reasonable steps that we can take to avoid this discrimination. We’re removing those reasonable steps.
Reading the ibn it seems that the CMFO was doing this as a favour to HQAC & now after a rearrangement (or a civvy subcontract?) it’s a task that wasn’t accounted for.
Possible solutions - adopt the civilian standards for AEF & scholarships/solo go through the medical board.
Currently many of these conditions, after discussion with the CFMO, will not stop cadets flying. Now, all cadets who meat any of these can’t fly, at all.
I think the point would be that they require a professional to ascertain whether or not they’re a risk.
Considering so few people understand things like ASD, or what it means to have had certain medications on that list (likely an issue because they cause drowsiness), then an inability to assess would leave us vulnerable when the point of these flights is to give cadets supervised control or an aircraft.
I’m going down a rabbit hole tangent as the only thing searchable is the CAA but their advice that you always need an AME sign off for autism but for adhd it’s the medication rather than the condition itself.
They’ve shot themselves in the foot here. All I’m going to do is send any cadet who meets that criteria, or who has a short time left on their current 6424 a new one so the system is going to be overloaded.
anyone who is anyone suffering long term asthma is having this managed by an “oral steroid” - for those not up to speed - the blue inhaler is a reliever - used at the point of attack, while the brown inhaler is a daily use preventer - the prevention drug is a steroid, which as you might imagine being an inhaler is taken orally…
they [HQAC] obviously mean oral tablets (as these are short term solutions often following a serious attack or prologue period of attacks) rather than common, routine, daily medication but that isn’t what the form says…!
AvMed 1 was updated a few revisions ago to clarify they mean tablets not inhalers:
Has the Cadet used oral steroids (tablets not inhaler) or antibiotics to treat Asthma within the last 6 months?
But confusingly the box below then says (my bold):
Does the Cadet have Asthma which is not stable (STEP 3 or above)? This includes the use of long-acting beta agonists, oral treatments or high-dose steroids.
Wouldn’t inhalers count as oral treatment? And that’s not withstanding the point that if it does get to F6424 it doesn’t differentiate for the GP between inhalers and tablets, so will likely end up going to CFMO anyway. Maybe this is part of the reason their withdrawing support - lots of requests for cadets with asthma but preventative inhalers
However worth noting that CAA does have different medical standards to the RAF/MAA. For example a cadet can in most cases hold a CAA Class 2 medical for an allergy with an EpiPen, but their RAF F6424 (and now AvMed 1 since the latest update) restricts them to ghosted solo because of MOD policy
Frequently a trigger for Asthma is a chest infection, which requires antibiotics and a short course of oral steroids, starting with a large dose which tappers off to zero over subsequent days. The lag effect of chest infections can last many weeks.
Long term steroid use in children is best avoided due to the side effects of prolonged use.